

By Wilson Catapani
Carnival, Brazil’s most vibrant and eagerly awaited celebration, is a time of pure joy, release, and cultural expression for millions of people. However, amid this excitement, there is a frequent companion that, when consumed without moderation, can transform the festivities into a scenario of serious health and safety problems: alcohol.
Our purpose here is to reflect on the hidden price excessive alcohol consumption demands from us — a cost that extends far beyond a simple hangover and deeply impacts both individuals and society.
The atmosphere of “freedom” and “relaxation” during Carnival is often misunderstood as permission to drink without limits. What begins as a celebration can quickly evolve into a troubling situation, overloading hospitals and police stations alike.
Alcohol, a psychoactive substance, acts directly on the central nervous system, impairing vital brain functions. It affects the prefrontal cortex, responsible for reasoning and judgment, and the cerebellum, which controls motor coordination. As a result, logical thinking, movement coordination, and reaction speed become compromised. Under the influence of alcohol, we — and consequently those around us — become far more vulnerable to accidents, risky situations, and impulsive decisions.
The drinking pattern known as binge drinking (heavy alcohol consumption within a short period) is particularly common and dangerous during this season.
It is alarming to observe the traffic accident statistics reported by Brazil’s National Traffic Department (DENATRAN) and law enforcement agencies during Carnival. In major urban centers such as São Paulo and Rio de Janeiro, the number of accidents involving serious injuries and deaths may increase by approximately 20% to 40%.
Drinking and driving emerges as the leading cause in more than 60% of these incidents. Alcohol impairs peripheral vision, reduces the ability to judge distances and speeds, and creates a false sense of confidence, turning drivers into immediate dangers on the road.
The strict enforcement campaigns under Brazil’s Lei Seca (“Dry Law”), which result in thousands of drivers being fined, losing their licenses, or even facing criminal charges, are undeniable evidence of the seriousness and persistence of this entirely preventable problem.
The euphoria induced by alcohol — often deceptive — can easily turn into aggression. Reduced inhibition and diminished impulse control significantly increase the risk of fights, robberies, and, most seriously, cases of sexual and domestic violence.
Epidemiological studies indicate that alcohol is involved in approximately one-third of interpersonal violence cases and plays a crucial role in many incidents of violence against women, where the ability to provide consent is frequently compromised by intoxication, whether on the part of the victim, the aggressor, or both.
In addition, intoxication makes people easier targets for crimes such as theft, robbery, and scams, as criminals take advantage of impaired perception and reaction abilities. This escalation of violence not only causes profound personal harm but also overloads public security and justice systems.
Beyond social and safety impacts, excessive alcohol consumption places a heavy burden on the body.
Hospitals and emergency care units experience a sharp increase in admissions during Carnival, many directly related to alcohol abuse. These cases not only constitute medical emergencies themselves but also divert resources and attention from other urgent conditions.
Rapid consumption of large amounts of alcohol can lead to severe alcohol poisoning. Blood alcohol concentration rises to dangerous levels, affecting vital functions.
Symptoms may progress from confusion and disorientation to stupor, loss of consciousness, respiratory difficulties, uncontrollable vomiting with aspiration risk, and, in extreme cases, coma or death. In some Brazilian capitals, emergency visits for this condition rise between 50% and 70% during Carnival.
Alcohol has a strong diuretic effect, increasing fluid loss. Combined with intense heat and prolonged physical activity during festivities, dehydration can lead to dizziness, severe headaches, muscle cramps, exhaustion, and even heatstroke from prolonged sun exposure.
People with preexisting conditions such as heart disease, diabetes, or respiratory disorders face even greater risks, including health crises or decompensation.
The liver is the primary organ responsible for metabolizing alcohol through enzymes such as alcohol dehydrogenase. When overloaded, it can suffer significant damage.
A single episode of excessive drinking may trigger acute inflammation (alcoholic hepatitis), characterized by jaundice, fever, nausea, abdominal pain, and fatigue. For chronic drinkers, each binge episode accelerates the progression of long-term liver diseases such as fatty liver disease and cirrhosis.
Alcohol directly irritates the lining of the stomach and esophagus, causing acute gastritis and esophagitis. Symptoms include severe heartburn, burning sensations, nausea, and persistent vomiting lasting for days.
Individuals with preexisting gastroesophageal reflux disease may experience significant worsening of symptoms.
Excessive alcohol consumption is one of the possible causes of acute pancreatitis, a potentially severe inflammatory condition of the pancreas. It can result in intense abdominal pain, nausea, vomiting, fever, and, in severe cases, complications such as tissue necrosis and multiple organ failure.
“Post-Carnival depression” is a reality for many people. Although alcohol may initially create feelings of euphoria, it is ultimately a depressant of the central nervous system.
It disrupts neurotransmitters such as serotonin and dopamine, intensifying anxiety, sadness, irritability, and dysphoria during withdrawal periods. Individuals with preexisting mental health disorders may experience relapses or worsening symptoms.
Additionally, alcohol abuse during Carnival may trigger the development or worsening of alcohol dependence.
Given all these risks, the major challenge is balancing the excitement of the celebration with the protection of our health and safety. The good news is that it is entirely possible to fully enjoy Carnival without falling into excess.
Prevention, moderation, and self-care are the keys to a truly safe celebration.
For a mindful reveler, preparation begins long before leaving home:
Alternate every alcoholic drink with a glass of water. This is crucial to counteract alcohol’s diuretic effects and Carnival’s intense heat, helping prevent dehydration.
Coconut water, sports drinks, and natural juices are also excellent choices for replenishing electrolytes and nutrients.
Never drink on an empty stomach. Eat nutritious and balanced meals before and during festivities.
Foods rich in protein and complex carbohydrates (such as whole grains and lean meats) help slow alcohol absorption and minimize its effects.
The primary goal is celebration and enjoyment — not intoxication.
Set a personal drinking limit before you begin and try to stick to it. Savor the event and the company around you. Avoid mixing different types of alcoholic beverages, as this may make it harder to monitor intake and accelerate intoxication.
Your body and mind need time to recover. Ensure adequate sleep and relaxation between days of celebration to maintain energy and mental clarity.
This rule is non-negotiable.
Use taxis, ride-sharing apps, public transportation, or designate a sober driver. Everyone’s life on the road is far too valuable to risk because of an irresponsible decision.
Use sunscreen with a high protection factor, wear sunglasses, hats or caps, and light clothing. Seek shaded areas whenever possible.
This protection not only prevents sunburn and heatstroke but also reduces physical exhaustion that may encourage additional drinking.
Persistent headaches, severe nausea, excessive dizziness, or any unusual discomfort are warning signs. Listen to your body and reduce or stop drinking.
If symptoms become severe or persistent, seek medical attention immediately.
Carnival, at its core, reflects our society. The way we celebrate — especially regarding alcohol consumption — has a direct and profound impact on public health, collective safety, and individual well-being.
This is not about restricting joy or prohibiting fun, but rather about cultivating celebration in a sustainable, conscious, and responsible way.
Data and lived experiences clearly show that irresponsible alcohol use leaves deep scars, increasing accidents, violence, and critical strain on healthcare systems.
We should strive to move beyond temporary euphoria and reflect on the choices we make. True freedom lies in the ability to care for ourselves and protect others.
May the hangover — if it comes — remain only a minor inconvenience, and not a heavy debt against our health and our lives. Carnival can and should be a celebration of conscious joy, respect for the body, and appreciation for life in its fullest sense.
By Lara Natacci
Holiday celebrations often bring together friends, family, special meals, and, frequently, alcoholic beverages. During these periods, alcohol consumption tends to increase, and understanding how to make safer choices is essential — especially because alcohol is a psychoactive substance capable of affecting different body systems, with risks that vary according to the amount consumed, the context, and individual characteristics.
Healthcare professionals and consumers both play an important role in this scenario: recognizing that alcohol is part of many people’s lives and, from that perspective, promoting realistic strategies for moderation and harm reduction.
The effects of alcohol depend mainly on the volume consumed, regardless of the type of beverage. Excessive use is associated with an increased risk of more than 200 diseases and health conditions, including accidents, metabolic changes, liver problems, and certain types of cancer. Even in the short term, symptoms such as dehydration, reduced motor coordination, cognitive impairment, and falls become more common.
During the holidays, the combination of disrupted sleep routines, irregular eating habits, and consecutive social events can intensify these effects. That is why planning ahead is essential.
Some simple measures can help reduce alcohol-related negative effects:
Avoid drinking on an empty stomach. Foods rich in fiber, protein, and healthy fats slow alcohol absorption.
Prioritize balanced meals. The Mediterranean dietary pattern — associated with long-term health benefits — includes moderate alcohol consumption alongside meals, with slow eating, social connection, and mindful attention to the moment.
Be cautious with sugary drinks. Sweet cocktails, liqueurs, and mixed drinks may increase blood sugar spikes and encourage greater alcohol intake than originally planned.
Stay hydrated. Alternating each alcoholic drink with water or other non-alcoholic beverages reduces dehydration and helps control total consumption.
The alcohol-free beverage market has expanded and now offers sensory experiences closer to the original products. For people who consume alcohol, alternating between alcoholic and non-alcoholic versions may help reduce the total amount consumed while maintaining social participation.
Studies reviewed by CISA indicate that this substitution does not increase alcohol consumption among non-drinkers and may significantly reduce intake among regular consumers.
However, these beverages should not be used by pregnant individuals, minors, abstainers, or people undergoing treatment for alcohol dependence.
The concept of Mindful Drinking has gained relevance in the context of harm reduction. The idea is simple: bringing attention and presence to the act of drinking by recognizing motivations, physical sensations, and emotions.
A randomized study cited in our analyses showed that a brief mindfulness session (11 minutes) was able to reduce alcohol consumption over the following week among at-risk drinkers. This reinforces that small self-awareness strategies can have a real impact.
Pause before the first sip. Ask yourself: “Am I drinking for pleasure, habit, impulse, or social pressure?”
Assess hunger, thirst, fatigue, or stress — factors that may lead to automatic consumption.
Decide in advance how much you intend to drink and in which situations.
Set realistic and achievable goals. Moderation is more successful when goals are practical and adapted to real life.
Examples:
Define a limit: “Two glasses of wine at dinner.”
Alternate drinks: “Drink one glass of water between each alcoholic beverage.”
Plan for common obstacles: availability of non-alcoholic beverages, the pace of the celebration, and peer influence.
Achievable goals increase confidence and reduce the likelihood of drinking more than intended.
The relationship between alcohol, lifestyle, and health involves multiple factors. For this reason, conversations free of judgment and grounded in empathy and accessible language help people recognize their challenges and find safer paths forward.
The holiday season is a time for celebration, but also an opportunity to practice responsible choices. The combination of proper nutrition, hydration, alternating with non-alcoholic beverages, clear goals, and Mindful Drinking practices contributes to experiencing festivities with greater well-being and safety.
Moderation does not mean giving up pleasure or social connection, but rather allowing these moments to create good memories — without negative consequences for health.
The Pan American Health Organization (PAHO) recently published a new report on Alcohol and Health in the Americas (2025),¹ compiling WHO (2024) data on alcohol consumption, mortality, and alcohol-related harms across 35 countries in the region. The document warns that alcohol continues to be a major preventable risk factor for disease, violence, and premature death, while also highlighting that public control policies are still progressing too slowly and insufficiently in light of the severity of the problem in the Americas.
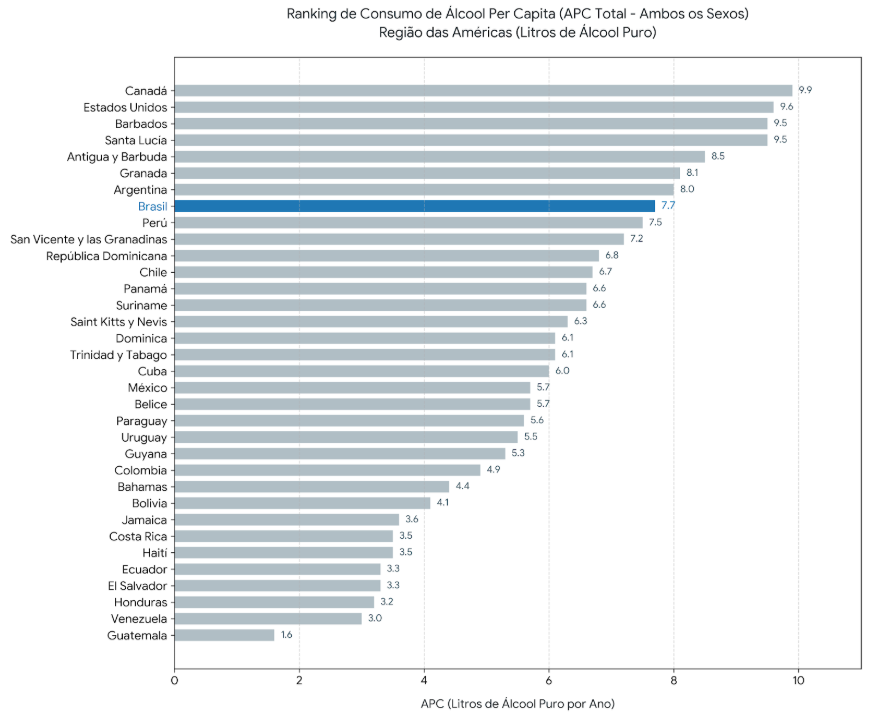
According to the new PAHO report, the Americas remain among the regions with the highest alcohol consumption in the world. The region maintains an average consumption of more than 7 liters of pure alcohol per capita per year, ranking second globally behind only Europe.
The data also show that more than 60% of the adult population in the region regularly consumes alcoholic beverages. Among the countries with the highest per capita consumption are Canada (9.9 liters), the United States (9.6 liters), and Barbados (9.5 liters). Brazil ranks eighth (7.7 liters).
The pattern of heavy episodic drinking (binge drinking) is also concerning. In 2019, the average prevalence of binge drinking episodes in the general population of the Americas was 25.7%, reaching 35.9% among men and 15.8% among women.
Among adolescents aged 15 to 19, the situation is particularly alarming: alcohol consumption prevalence reached 41.9%, making the Americas the region with the second-highest alcohol consumption in this age group worldwide. The report states that these numbers are “unacceptably high,” especially considering the risks to brain and neurocognitive development and the existence of laws prohibiting alcohol sales to minors.
Another relevant finding is the predominance of beer as the most consumed alcoholic beverage in the Americas: it accounts for 53.8% of recorded alcohol consumption in the region, a proportion higher than in any other WHO region.
The PAHO report reinforces that alcohol is associated with more than 200 health conditions, including cardiovascular diseases, cancers, liver cirrhosis, mental disorders, violence, and traffic accidents.
In the Americas, alcohol consumption was responsible for approximately 385,354 deaths in 2019, including 318,412 among men and 66,942 among women.
The burden of alcohol-attributable disease also remains high. The region recorded 32.7 deaths and 1,747 disability-adjusted life years (DALYs) lost per 100,000 inhabitants, placing the Americas among the most affected regions in the world.
Among the main alcohol-related harms are:
The document also highlights that the impact of alcohol extends beyond individual health, affecting families, communities, economic productivity, and global sustainable development goals.
Among the report’s central recommendations is strengthening the so-called SAFER policies, the WHO technical package aimed at reducing harmful alcohol use. In this context, PAHO highlights higher taxes and minimum pricing policies as some of the most cost-effective interventions available to governments.
According to the report, fiscal policies reduce the economic affordability of alcoholic beverages, especially among young people and groups more vulnerable to harmful consumption. In addition, such measures can generate additional revenue for public health investments and prevention programs.
Despite this, adoption of these measures remains limited across the Americas. Many countries still maintain outdated tax structures without inflation adjustments or mechanisms capable of effectively reducing consumption.
Regarding Brazil, the data show that the country remains above the global average in alcohol consumption, recording 7.7 liters of pure alcohol per capita in 2019.
In addition, according to the report:
The document also projects growth in Brazilian alcohol consumption through 2030, reinforcing the need to strengthen public prevention and regulatory policies.
The data presented by PAHO reinforce that harmful alcohol consumption remains one of the greatest public health challenges in the Americas. The combination of high consumption prevalence, early initiation, easy access, and still-insufficient regulatory policies contributes to the persistence of a high burden of preventable diseases and deaths.
In this context, expanding access to high-quality scientific information and strengthening evidence-based policies become essential measures to reduce harm, protect vulnerable populations, and support public health decision-making.
References:
Organização Pan-Americana da Saúde (OPAS). Informe sobre la situación del alcohol y la salud en la Región de las Américas 2025. Washington, DC: OPAS; 2025. Disponível em: OPAS. Acessed: May 22, 2026.
Chronic pain affects about one in every three adults, and many of these individuals seek relief in a widely available substance: alcohol. What few people realize is that this shortcut may conceal a biological trap capable of turning temporary pain into prolonged suffering and opening the door to alcohol use disorder.¹
Research shows that up to 38% of heavy drinkers report using alcoholic beverages to relieve physical pain.¹ And this phenomenon is not merely cultural: scientific studies confirm that alcohol does, in fact, have some analgesic effect. The crucial detail, however, is that this relief only appears at high doses — around 0.08 g/dL of blood alcohol concentration — the same level that characterizes binge drinking, defined as four or more drinks on a single occasion for women and five or more for men, a pattern associated with several diseases and health complications such as cancer, hypertension, and alcoholism itself.² ³
The problem is that this analgesic effect is brief and deceptive. Within just a few hours after consumption, acute tolerance sets in: the body responds less and less to the same amount of alcohol. Even worse, as alcohol leaves the system, sensitivity to pain does not simply return to normal — it may become amplified in a phenomenon known as hyperalgesia. In other words, the next day, or during periods of abstinence, a person may feel more pain than they would have if they had never consumed alcohol in the first place.¹
Alcohol provides temporary comfort from pain but leaves the individual even more vulnerable shortly afterward. The brain quickly learns that “another drink” may bring relief, creating an urge to drink again, in increasingly larger amounts and at increasingly shorter intervals.¹ ⁴
Over time, intense and prolonged alcohol consumption causes lasting changes in the central nervous system, making the brain more sensitive to pain (a process called central sensitization) and potentially causing direct damage to peripheral nerves, known as alcoholic neuropathy. It is no coincidence that people with alcohol use disorder report chronic pain at much higher rates (43% to 54%) than those who drink little or not at all (28% to 33%).¹ What began as an attempt to cope with pain becomes, itself, a new source of suffering and a major obstacle to recovery, since higher levels of pain are associated with a greater risk of relapse among those seeking treatment.¹
The good news is that effective and safe alternatives do exist. Psychological approaches such as cognitive behavioral therapy (CBT) and mindfulness-based interventions have shown promising results in the combined management of pain and alcohol consumption.¹ Certain medications already used in the treatment of alcohol use disorder, such as naltrexone, topiramate, and gabapentin, may also have beneficial effects on chronic pain and can be valuable options when prescribed by a healthcare professional. Recognizing that alcohol is not a remedy for pain and seeking proper medical evaluation to treat the underlying problem is the first step toward breaking free from this cycle.
References:
Women and Alcohol: The Importance of Brief Intervention in Primary Health Care, by Janaina Soares
Alcohol consumption among women has increased in recent decades, becoming an important public health issue. Historically, alcohol use was more prevalent among men, but social, cultural, and economic changes have contributed to narrowing this gap. This scenario demands greater attention from health services, especially Primary Health Care (PHC), which serves as the main entry point to the health system and plays a strategic role in the early identification and management of risky alcohol use among women.
According to Brazil’s Ministry of Health, one standard drink corresponds to approximately 10 grams of pure alcohol. In practice, this equals about 250 ml of beer, 100 ml of wine, or 30 ml of distilled spirits. In general, the higher the alcohol content of a beverage, the smaller the volume that corresponds to a standard drink.
For women, low-risk consumption is defined as up to one standard drink per day, with at least two alcohol-free days per week recommended. These intervals are important to reduce the development of tolerance—a phenomenon in which increasing amounts of alcohol are needed to achieve the same effects—which can contribute to progression toward dependence. For men, the low-risk limit is typically up to two drinks per day.
This difference is related to biological characteristics of the female body. In general, women have a lower proportion of body water, lower average body weight, and lower activity of the enzyme alcohol dehydrogenase in the gastric mucosa, which is responsible for part of alcohol’s initial metabolism. Since ethanol is distributed primarily in body water, these factors result in higher blood alcohol concentrations in women compared to men after consuming equivalent amounts.
Because of this greater systemic exposure, women are more vulnerable to alcohol’s effects and may develop health damage in a shorter period of time. Key consequences associated with alcohol use include liver and cardiovascular diseases, mental health disorders, increased risk of certain cancers, and significant impacts on reproductive health and pregnancy.
Beyond biological effects, alcohol consumption among women is also associated with important psychosocial factors. Work overload, violence, gender inequalities, psychological distress, anxiety, and depression can contribute to harmful drinking as a coping mechanism. In the context of pregnancy or reproductive planning, alcohol use poses additional risks, including adverse fetal outcomes such as fetal alcohol spectrum disorders.
In this context, brief intervention is an effective, low-cost, and widely applicable strategy for preventing and reducing risky alcohol consumption. It is a structured approach, typically delivered in just a few minutes during a consultation, involving targeted counseling, personalized feedback on drinking patterns, and encouragement of critical reflection on the risks associated with alcohol use. It also includes collaboratively developing a menu of options to address risky behavior and strengthening the individual’s self-efficacy to promote change.
It is essential that this approach be conducted in an empathetic and nonjudgmental manner, fostering a trusting environment where individuals feel comfortable discussing their alcohol use and related challenges. The healthcare professional’s attitude should encourage open dialogue and active listening, helping individuals reflect on their behaviors and consider possible changes.
This strategy can be carried out by different members of the healthcare team and has strong evidence supporting its effectiveness in reducing alcohol consumption, particularly among individuals who have not yet developed dependence.
In Primary Health Care, brief intervention can be integrated into routine women’s health visits, such as reproductive planning consultations, prenatal care, gynecological follow-ups, and health promotion activities. Systematic screening using standardized tools, such as the Alcohol Use Disorders Identification Test (AUDIT) or its abbreviated version (AUDIT-C), allows for the identification of risky drinking patterns and the direction of appropriate interventions.
Incorporating these strategies into PHC services contributes to more comprehensive care for women’s health, enabling not only early identification of harmful alcohol use but also strengthening the relationship between healthcare providers and patients. It also facilitates addressing other social and emotional determinants associated with alcohol use—such as caregiving burden, experiences of violence, psychological distress, and structural gender inequalities—promoting more holistic and gender-sensitive care.
Strengthening the capacity of Primary Health Care to conduct screening and brief interventions for alcohol use among women is a key strategy to prevent health problems, reduce harm, and promote better living conditions for the female population.
Legal Blood Alcohol Limits and Traffic Mortality: What Data from 165 Countries Reveal
Driving under the influence of alcohol remains one of the leading preventable causes of traffic deaths worldwide. It is estimated that about 27% of all road traffic fatalities are related to alcohol use, with a disproportionate impact on low- and middle-income countries.¹ Against this backdrop, researchers from Yale School of Medicine conducted a groundbreaking study analyzing 165 countries to understand how legal blood alcohol concentration (BAC) limits relate to alcohol-attributable traffic mortality rates, and which national factors influence this relationship.¹
The World Health Organization (WHO) recommends a maximum BAC limit of 0.05 g/dL for the general population and 0.02 g/dL for drivers. To give a practical sense, a 68 kg (150 lb) man reaches approximately 0.05 g/dL after consuming about three standard drinks over two hours, while women reach this level with significantly less alcohol due to biological differences in metabolism.¹ Despite these guidelines, the study found that around 51 of the 165 countries analyzed maintained limits above the WHO recommendation, highlighting a significant gap between scientific evidence and legislative practice.¹
Brazil, in this regard, ranks among the strictest countries: its “Lei Seca” (Dry Law — Law No. 11.705/2008, amended by Law No. 12.760/2012) establishes a zero-tolerance policy, meaning a BAC of 0.00 g/dL—going even further than WHO recommendations. In the study, countries with zero-tolerance policies were classified in the most restrictive category, and the data indicate that lower BAC limits are associated with lower traffic mortality rates.¹
One of the most revealing findings concerns differences between men and women. Men showed mortality rates about five times higher than women, and the relationship between higher BAC limits and increased deaths was significantly stronger among men. This reflects the fact that men are more likely to engage in risk behaviors such as heavy drinking and driving under the influence, making them disproportionately vulnerable when laws are more lenient.
Beyond the numeric legal limit, the study demonstrated that structural factors within each country strongly influence the effectiveness of traffic policies. Countries with lower national income, greater gender inequality, and higher per capita alcohol consumption had higher mortality rates. In low- and middle-income countries, challenges such as weak enforcement systems, lack of roadside alcohol testing equipment, and limited access to emergency medical care exacerbate the problem, meaning that even strict laws may have reduced real-world impact.
Healthcare infrastructure also plays a crucial role. Countries with stronger health systems—featuring robust emergency response capacity and coordinated trauma care—showed smaller gender disparities and a less steep relationship between BAC limits and mortality. This suggests that effective healthcare systems can act as a safety net, reducing deaths even when accidents occur, while also supporting prevention and public education efforts about the risks of drinking and driving.
The experience of some countries illustrates how integrated approaches can make a difference. Lithuania, for example, combined higher alcohol taxes, restricted sales hours, advertising bans, and expanded public health programs, resulting in significant reductions in traffic injuries and deaths between 2004 and 2019. Similarly, Scotland implemented a minimum unit pricing policy for alcohol in 2018, and within 32 months, alcohol-attributable deaths fell by 13.4%, with the greatest reductions seen among men and socioeconomically vulnerable populations.¹
The authors emphasize that public education campaigns should clarify that legal BAC limits are regulatory thresholds—not indicators of physiological safety. Measurable impairment in driving ability can occur even at lower concentrations, especially among women. In addition, recent global trends show increasing risky drinking behaviors among women, narrowing the historical gender gap in alcohol-related harm and requiring continued attention from public policy.
In summary, the study reinforces that lowering BAC limits is an important but insufficient measure when implemented in isolation. Maximizing reductions in traffic deaths requires that laws be accompanied by reliable enforcement, access to emergency care, reductions in per capita alcohol consumption, and targeted prevention strategies—particularly for male populations and countries with greater structural inequalities.¹ In the Brazilian context, these findings serve as an important warning: although the country’s zero-tolerance law places it among the most restrictive in the world, international evidence shows that legislation alone is not enough. Strengthening roadside enforcement, investing in emergency and trauma care, and promoting awareness campaigns—especially aimed at men, who are historically the most affected—are essential steps to ensure that zero tolerance on paper translates into lives saved in practice.
References:
Sports Betting and Excessive Alcohol Consumption: A Concerning Association
In recent years, sports betting has become widely accessible through apps and digital platforms, reaching millions of people. At the same time, scientific evidence has increasingly shown that this practice may be linked to riskier patterns of alcohol consumption.¹–⁵ A study published in JAMA investigated whether U.S. adults who bet on sports are at greater risk of episodic heavy drinking—commonly known as binge drinking—compared to the general population.
The study, conducted by Grubbs and Kraus (2024),¹ analyzed data from 4,363 adults living in the United States, collected between March and April 2022. The sample included both a representative portion of the general population and an additional group of sports bettors, allowing for robust comparisons between those who bet and those who do not. Excessive alcohol consumption was assessed using a questionnaire (National Institute on Drug Abuse Quick Screen), which defines binge drinking as consuming five or more drinks on a single occasion for men, and four or more for women.
Among participants, 1,812 were identified as sports bettors, and the profile of this group stood out: they were predominantly male and younger, with an average age of 45.8 years—about four years younger than the overall sample average. When examining the frequency of binge drinking, sports bettors showed disproportionately higher rates of excessive consumption on a monthly, weekly, and even daily basis, while less frequently reporting complete abstinence from binge drinking over the previous 12 months.
One of the study’s most striking findings concerns the magnitude of this association. In logistic regression analyses controlling for variables such as age and race/ethnicity, women who engaged in sports betting were about 14 times more likely to report daily or near-daily binge drinking compared to women who did not bet. Among men, this likelihood was approximately 9 times higher. Even at lower frequencies, such as weekly or monthly binge drinking, sports bettors of both sexes showed significantly higher odds compared to non-bettors, suggesting that the association between betting and excessive alcohol use is not limited to the most extreme cases.
Importantly, this pattern persisted even when compared to individuals who engaged in other forms of gambling not related to sports, such as slot machines, roulette, and lotteries. In other words, there appears to be something specific about sports betting that is linked to particularly risky alcohol consumption behaviors. Previous research has already suggested that sports bettors tend to have a higher propensity for risk-taking behaviors in general,⁵⁻⁶ which may help explain this finding.
The authors acknowledge some limitations of the study: its cross-sectional design does not allow for conclusions about causality (whether betting leads to excessive drinking or vice versa), and the use of online panel sampling methods may limit generalizability. Nevertheless, the findings are consistent with prior studies showing that sports bettors report more symptoms of alcohol use disorder.³⁻⁴
Given the rapid expansion of sports betting—driven by legalization in many U.S. states and, more recently, in countries like Brazil—these results underscore the urgent need for integrated public health policies. Understanding how new betting technologies influence the prevalence and presentation of alcohol-related disorders is essential to protect populations increasingly exposed to this dual risk.
Note: This text is for informational purposes only and is based on recent scientific studies. It does not replace professional medical advice.
References:
Episodic Heavy Drinking and Mortality in Older Adults: What a Large Canadian Study Teaches Us
Episodic heavy drinking, known as binge drinking, is not a behavior limited to young people. Among adults aged 50 and older, this practice has been increasing in recent decades, and its health consequences are more serious than many realize. A new Canadian study published in 2026 analyzed more than 129,000 adults and showed that those who frequently drink large amounts on a single occasion have a significantly higher risk of premature death, even after accounting for factors such as chronic diseases, overall health status, and lifestyle habits.
When discussing alcohol and aging, attention is usually focused on daily consumption, liver disease, or dependence. Binge drinking—defined as consuming four or more drinks on a single occasion for women, and five or more for men—is still commonly associated, in popular perception, mainly with adolescents and young adults. However, this perception is outdated. Recent research has shown that this pattern of drinking is actually increasing among older adults, and its health consequences are underestimated by both the public and healthcare systems.
It is within this context that a recent study published in the journal Alcohol by MacNeil and colleagues (2026)¹ stands out. Researchers from the University of Toronto used data from one of Canada’s largest national health surveys, the Canadian Community Health Survey, collected between 2005 and 2014 and linked to the country’s mortality database. The final sample included approximately 129,470 adults aged 50 or older who consumed alcohol at least once per month. Participants were followed until the end of 2017, allowing researchers to determine who died and when, and to compare these outcomes with the drinking patterns reported at the start of the study.
What the study measured
Participants were classified into four groups based on how often they reported binge drinking episodes in the previous year: never; less than once a month; one to three times per month; and once a week or more. The authors then applied survival analysis models, specifically Cox regression analyses, to estimate the risk of death associated with each pattern of consumption, progressively adjusting for sociodemographic factors (such as age, sex, income, and education) and health-related variables (including chronic diseases, self-reported health, smoking, physical activity, and mental health).
Of the participants, 60.1% reported no binge drinking episodes in the previous year. Another 21.2% drank this way less than once a month, 10.7% did so one to three times per month, and 8% reported heavy drinking at least once a week. Among those who died during the follow-up period (about 14,740 individuals), drinking patterns and health profiles differed significantly.
What the results showed
The study’s central finding is clear: older adults who engage in binge drinking at least once a week have a significantly higher risk of premature death than those who never drink this way. Even after adjusting for variables such as chronic diseases, smoking, physical inactivity, mental health, and socioeconomic status, individuals who reported no binge drinking in the past year had a 19% lower risk of death compared to frequent heavy drinkers. This is important because it shows that the association cannot be explained solely by the fact that people with more illnesses drink more, or that healthier individuals drink less. The drinking pattern itself carries an independent impact on mortality risk.
The study also identified a graded relationship: the more frequent the binge drinking, the higher the risk of death. Those who drank heavily less than once a month had a 17% lower risk than weekly binge drinkers; those who drank one to three times per month had a 12% lower risk. This dose–response pattern is an important epidemiological indicator, strengthening the argument that there may be a causal relationship—not just a statistical association—between binge drinking and premature mortality in older adults.
Why this matters for public health
To better understand this, imagine a study comparing people who drink moderately with those who do not drink at all. At first glance, it might seem that non-drinkers die earlier. However, there is a key detail: many people in the “abstainer” group stopped drinking because they were already ill. This creates a misleading impression—known as the “sick quitter bias”—that non-drinkers are less healthy, when in fact the group includes individuals who already had poor health and stopped drinking for that reason.
To address this issue, the researchers focused only on people who already consumed alcohol, avoiding comparisons with lifelong abstainers or those who quit due to illness. They also adjusted for self-reported health status. Even after removing this confounding factor, the data showed that binge drinking (consuming large amounts in a short time, such as “getting drunk” on weekends) remains a real risk to life, regardless of other factors. Excessive alcohol consumption does, in fact, shorten lifespan.
Another important point is that the study highlights a group often overlooked in public health campaigns: adults over 50 who drink heavily. Data cited by the authors show that binge drinking increased by 19% among Americans aged 50 and older between 2005 and 2014. In Brazil, where population aging is advancing rapidly and alcohol is deeply embedded in the culture, this discussion is urgent.
Specific risks of binge drinking in older age
The bodies of older adults do not metabolize alcohol in the same way as younger individuals. The proportion of body fat increases with age, while water content decreases, leading to higher blood alcohol concentrations even with similar amounts consumed. In addition, liver metabolism becomes less efficient, and the presence of multiple chronic conditions along with the use of medications increases the risk of harmful interactions. Falls, fractures, acute cognitive impairment, and drug interactions are particularly concerning in this age group, and binge drinking—due to its concentrated consumption pattern—amplifies all of these risks at once.
What to do with this information
The study’s authors rightly argue that alcohol-related interventions have focused too heavily on young people and acute risks such as accidents and violence, while neglecting the chronic effects on older adults. Family physicians and geriatricians play a central role in changing this: systematic screening of alcohol consumption patterns among patients over 50 remains underutilized in clinical practice. Asking about how a person drinks—not just whether they drink—should be a routine part of medical consultations.
There is also an important cultural dimension to this issue. Excessive alcohol consumption among older adults is often normalized or even romanticized as part of an active social life in later years. At the same time, stigma surrounding alcohol problems in this age group may lead both patients and healthcare professionals to avoid the topic. Breaking this invisibility is essential for ensuring that interventions reach those who need them.
Finally, it is worth noting that the study does not advocate total abstinence as the only solution. The authors recognize the importance of meeting people where they are and supporting any reduction in drinking patterns, rather than demanding immediate radical change. Reducing the frequency of binge drinking—even without completely eliminating alcohol consumption—already represents a meaningful health benefit. This is a more practical and humane perspective than messages based solely on abstinence, and it is exactly the kind of approach public health needs when addressing alcohol use and aging.
In summary, the study indicates that:
References:
Alcohol and Anabolic Steroids
The use of anabolic steroids is often associated with the pursuit of physical performance and aesthetic changes, while alcohol consumption is frequently seen as routine and socially acceptable. However, combining the two raises a warning sign. More recent studies show that, although there are still gaps in understanding the exact mechanisms of this interaction, the concurrent use of alcohol and anabolic steroids may increase the burden on the liver and be part of a broader context of risk behaviors, with consequences that go beyond liver health and include cardiovascular, hormonal, and psychiatric effects.
The non-medical use of anabolic androgenic steroids has grown in various contexts, far beyond professional sports. Today, this use is seen among gym-goers, amateur bodybuilders, and individuals motivated by aesthetic changes or improved physical performance. At the same time, alcohol remains one of the most widely consumed psychoactive substances in the world. When these two exposures overlap, an important public health concern arises: the potential combined effect on the body, especially on the liver¹.
Anabolic steroids alone are already associated with a range of adverse effects. Among the most well-known are hormonal changes, infertility, acne, gynecomastia, increased blood pressure, and mood changes. The liver is also a major concern. Recent reviews show that prolonged use at supraphysiological doses can lead to elevated liver enzymes, cholestasis, hepatic vascular alterations, and even benign or malignant liver tumors in some cases².
Alcohol, in turn, also has toxic effects on the liver and is associated with a broad spectrum of damage, ranging from steatosis to more severe forms of liver disease³. When a potentially hepatotoxic substance such as anabolic steroids is used in an organism already exposed to harmful alcohol consumption, clinical concern becomes even greater.
One of the most well-known studies on the topic analyzed data from the Drug-Induced Liver Injury Network (DILIN) in the United States, focusing on patients with drug-induced liver injury. The authors observed that among individuals with heavy alcohol consumption, anabolic steroids were prominent among the identified causes of drug-induced liver injury. This finding is relevant because it suggests that heavy alcohol use may be more common in groups where anabolic steroids already represent a risk factor for liver damage.
At the same time, the study raised an important point: the authors did not find clear evidence that heavy drinkers necessarily had worse final outcomes—such as liver-related death or the need for transplantation—compared to non-drinkers in that cohort. This does not mean the combination is safe. In practice, the findings suggest that the relationship between alcohol and anabolic steroid–related liver injury is complex and likely involves both biological and behavioral factors.
This point deserves attention. Part of the association between alcohol and anabolic steroids may reflect a broader context of risk behaviors, such as using substances without prescription, high-dose cycles, combining different compounds, and limited medical supervision²⁴. In other words, it is often not just the sum of two potentially harmful agents, but a pattern of use that already increases vulnerability to multiple health problems.
Recent literature also reinforces that the adverse effects of anabolic steroids extend far beyond the liver. A meta-analysis published in 2025 showed that abuse of these substances among athletes and physically active individuals is associated with significant increases in blood pressure and LDL cholesterol, highlighting their cardiovascular impact⁴. This broadens the discussion: individuals who use anabolic steroids and consume excessive alcohol may be exposing themselves to a combination of hepatic, metabolic, and cardiovascular risks simultaneously.
Another recent review highlighted that androgen abuse is associated with increased mortality and multisystem adverse effects, including cardiovascular toxicity, infertility, hypogonadism, hepatotoxicity, and mental health disorders³. This helps dispel the idea that anabolic steroids produce only “aesthetic” or “hormonal” effects. In reality, these substances can have wide-ranging impacts on the body, especially when used outside a medical context.
It is also important to distinguish between supervised therapeutic use and non-prescribed use. Recent studies show that individuals who use anabolic steroids without medical indication experience more adverse events than those undergoing clinically supervised testosterone therapy. This reinforces that risk is particularly concentrated in recreational, aesthetic, or performance-oriented use—often done without clinical monitoring, regular testing, or appropriate dosing, and sometimes involving unsafe combinations.
From a mental health and behavioral perspective, this combination also warrants caution. Recent reviews describe associations between anabolic steroid abuse and mood changes, aggression, impulsivity, and other psychiatric effects. Since alcohol is also linked to reduced self-control and increased exposure to accidents, violence, and risky decisions, the combination of these substances should not be viewed solely as a liver issue, but as a broader health concern.
From a prevention standpoint, the main message is clear: although more studies are needed to precisely define the biological interaction between alcohol and anabolic steroids, the existing body of evidence is sufficient to treat this combination with seriousness. It is not a trivial combination, especially when it involves heavy alcohol consumption, prolonged steroid use, oral compounds, and lack of medical supervision.
In summary, current evidence indicates that:
Informing the public about these risks is essential to counter the normalization of anabolic steroid use and excessive alcohol consumption. In public health, waiting for absolute certainty about every mechanism before issuing warnings is often a mistake. When signals of harm are already consistent, prevention remains the best course of action.
References:
Pancreas Under Pressure: The Silent Enemy of Alcohol Excess
For a long time, science has tried to unravel a major mystery: why does only a small minority of people who drink large amounts of alcohol develop acute pancreatitis?¹ The answer tells an intriguing story about how our bodies react to excess. It is important to emphasize that alcohol-related acute pancreatitis is strongly associated with chronic, heavy alcohol consumption. Moderate or occasional drinking does not cause pancreatitis. Prolonged heavy drinking leads to changes that make the pancreas vulnerable to an acute crisis.
Alcohol itself, or even the substances produced when the body processes it, cannot cause the disease on their own.² Instead, intense and prolonged alcohol consumption acts silently, reducing the pancreas’s natural chemical signaling and causing its fluids to become highly concentrated, acidic, and thick.
This situation is worsened because long periods of alcohol use are often accompanied by poor nutrition and low water intake.¹ This dehydration and relative fasting contribute to the formation of “sludge” or small protein plugs that temporarily block the tiny ducts through which pancreatic and bile fluids should flow. The danger may also arise when a person stops drinking, because after interrupting alcohol consumption and returning to normal eating—especially heavier or fatty foods—the body sends a strong signal and overstimulates the pancreas, which had been operating at a reduced pace.³ It is not the interruption of drinking or the return to normal eating that causes the crisis; rather, the crisis is triggered by the heavy alcohol intake that occurred beforehand.
Imagine a hose running at maximum pressure but with its end blocked. This is essentially what happens in the pancreas: it is forced to produce and secrete digestive juices intensely against blocked ducts.¹ Unable to flow out, these enzymes begin to act within the organ itself, effectively digesting pancreatic tissue, damaging cells, and triggering a cascade of severe inflammation. To make matters worse, continuous alcohol use weakens the pancreas’s natural defense mechanisms against this stress—an effect that is even stronger in people who also smoke.⁴
Symptoms of acute pancreatitis (severe abdominal pain, nausea, vomiting) may not appear immediately after the last drink. Pain can occur hours—or even one or two days—after excessive alcohol intake. During this interval, the person may have already stopped drinking and even tried to eat normally before symptoms become severe enough to require hospitalization. Returning to a normal diet, especially one high in fat, may simply worsen the symptoms of an already developing pancreatitis.
Acute pancreatitis is a serious medical emergency, and although medicine continues to search for treatments that can halt the disease at its origin, rapid diagnosis combined with intensive hospital support remains the most effective and safest way to stabilize the patient and save their life.
References









